
 Systematic reviews (SRs) are the embodiment of the evidence-based approaches, and they have reformed clinical decision-making in almost all therapy areas. The approach of SRs was essentially developed to fulfil the need of the medical practitioners to obtain precise and consistent information about the efficacy and safety of a clinical intervention, diagnostic procedure, or a prognostic marker from a pool of evidence, which is apparently full of contradiction, heterogeneity and bias.(1) Although SRs and meta-analyses are robust and detail-oriented, they’re both resource intense, with a limited scope of outcomes.(2) In order to cater to a range of needs from the stakeholders, the SR approach has branched within the realm of evidence synthesis. For instance, rapid reviews provide for more urgent deadlines but may not follow all the methods of an SR,(3) scoping reviews include larger bodies of evidence, not requiring a detailed synthesis,(4) and realist reviews focus on the assessment of the functions of complex interventions, often comprising of evidence excluded from classic SRs.(5, 6)
Systematic reviews (SRs) are the embodiment of the evidence-based approaches, and they have reformed clinical decision-making in almost all therapy areas. The approach of SRs was essentially developed to fulfil the need of the medical practitioners to obtain precise and consistent information about the efficacy and safety of a clinical intervention, diagnostic procedure, or a prognostic marker from a pool of evidence, which is apparently full of contradiction, heterogeneity and bias.(1) Although SRs and meta-analyses are robust and detail-oriented, they’re both resource intense, with a limited scope of outcomes.(2) In order to cater to a range of needs from the stakeholders, the SR approach has branched within the realm of evidence synthesis. For instance, rapid reviews provide for more urgent deadlines but may not follow all the methods of an SR,(3) scoping reviews include larger bodies of evidence, not requiring a detailed synthesis,(4) and realist reviews focus on the assessment of the functions of complex interventions, often comprising of evidence excluded from classic SRs.(5, 6)
Given the resource intense nature of the SRs, it is essential to recognize the most informative research questions in order to maximize their value and efficiency in clinical and regulatory decision-making. It can be inefficient to invest resources in SRs barely as a means of addressing specific research questions, if data available to answer those questions is lacking. Therefore, decision-makers need to monitor and understand the evidence base as a whole, so as to quickly determine the emerging trends or issues of potential concern. This can, in turn, facilitate the development of proactive research questions by relevant stakeholders for SRs to answer.(1)
Evidence mapping is a new approach for the evidence review process. This approach can potentially expedite evidence surveillance in a clear and reproducible manner, thus offering a broader understanding of the existing evidence base through interactive yields.(1) Evidence maps and evidence visualizations are systematic evidence synthesis approaches, which work by displaying visually the gaps in evidence or study characteristics, and, at times, summarize study quality or synthesized evidence from multiple studies. Such an interactive and visual representation provides a quick overview of the existing evidence base, thereby helping stakeholders and researchers to immediately understand research priorities.(7) For these reasons, evidence maps are excellent tools that help in guiding clinical investigators to set the agenda for future research.(8)
Being a rather new concept, there has been no uniform definition of, or methodology for conducting, evidence maps yet. Mainly, evidence maps are referred to as tools of systematic organisation and illustration of evidence base with the intent to characterize the breadth, depth and methodology of relevant evidence, identifying gaps.(9) Another definition of evidence map is “an approach to providing a visual representation and critical assessment of evidence landscape for a particular topic or question”.(10) A more recent definition is developed from the published evidence maps, which turned out to be a systematic search of a broad field identifying gaps in knowledge and the needs for future research.(6) The last one thus takes evidence maps to be a user-friendly representation of evidence bases visually in a figure or graph, a table or a searchable database.(8)
Nonetheless, due to the lack of a uniform definition, the stakeholders may not essentially know what to expect while warranting an evidence map or identifying existing maps. Moreover, lack of a repository for evidence maps makes them difficult to locate, thus making it less likely for authors to develop existing approaches further.(11)
Essentially, evidence maps are primarily prepared by the relevant stakeholders (researchers, policy-makers, funders, and, most importantly, patients) by identifying the most important clinical questions to their context, and researching on the body of evidence that is available already. Next, the quality of the available evidence is assessed and conveyed to stakeholders. The final step includes the visual depiction of the most relevant data elements to the stakeholder; for e.g., focusing on the size of the body of evidence, comparisons made versus those avoided, populations studied versus those avoided, and risk of bias, among other factors.(8) At the end of this process, the gaps in the available evidence in the context of the original research question starts to become apparent, and this can be used to plan further research activities.
In conclusion, evidence maps offer a robust and transparent methodological framework with which to assess the evidence landscape in a detailed manner, and aid clinical and regulatory decision-making. The broad scope of evidence maps, through efficient use of resources, can substantially streamline evidence synthesis by preventing unnecessary duplication of work. Additionally, future text mining and machine learning advancements will further possibly reduce the resource intensity of the methodology.(8)
Become A Certified HEOR Professional – Enrol yourself here!
References
- Wolffe TAM, Whaley P, Halsall C, et al. Systematic evidence maps as a novel tool to support evidence-based decision-making in chemicals policy and risk management. Environ Int. 2019; 130:104871.
- Bastian H, Glasziou P, Chalmers I. Seventy-five trials and eleven systematic reviews a day: how will we ever keep up? PLoS Med. 2010; 7(9):e1000326.
- Tricco AC, Antony J, Zarin W, et al. A scoping review of rapid review methods. BMC Med. 2015; 13(1):224.
- Colquhoun HL, Levac D, O’Brien KK, et al. Scoping reviews: time for clarity in definition, methods, and reporting. J Clin Epidemiol. 2014; 67(12):1291–4.
- Pawson R, Greenhalgh T, Harvey G, et al. Realist review–a new method of systematic review designed for complex policy interventions. J Health Serv Res Policy. 2005; 10 suppl 1:21–34.
- Miake-Lye IM, Hempel S, Shanman R, et al. What is an evidence map? A systematic review of published evidence maps and their definitions, methods, and products. Syst Rev. 2016; 5:28.
- Evidence Maps and Evidence Visualizations. Patient-centered Outcomes Research Institute. Available at: https://www.pcori.org/impact/evidence-maps-and-evidence-visualizations
- Alahdab F, Murad MH. BMJ Evidence-Based Medicine. 2019.
- Katz DL, Williams AL, Girard C, et al. The evidence base for complementary and alternative medicine: methods of Evidence Mapping with application to CAM. Altern Ther Health Med 2003; 9:22–30.
- Bethan C, O’Leary PW, Kaiser MJ, et al. Evidence maps and evidence gaps: evidence review mapping as a method for collating and appraising evidence reviews to inform research and policy. Environmental Evidence 2017; 6.
- Evidence and gap maps: A comparison of different approaches. Oslo, Norway: The Campbell Collaboration. Retrieved from: campbellcollaboration.org/ DOI: https://doi.org/10.4073/cmdp.2018.2

 Clinical practice should ideally rely on robust scientific evidence, the standard for which are systematic reviews and meta-analyses of all randomised controlled trials (RCTs). (1,2) Therapeutic decisions in healthcare must be informed by clinical research findings, and patients and prescribers must be able to trust the presented research evidence. However, this evidence can be considered valid only if the studies included in reviews and meta-analyses signify the complete publications, without any bias. (2) Recently, the reliability of much of the evidence base for several popular therapeutic and preventive interventions has been challenged due to the publication bias. (3)
Clinical practice should ideally rely on robust scientific evidence, the standard for which are systematic reviews and meta-analyses of all randomised controlled trials (RCTs). (1,2) Therapeutic decisions in healthcare must be informed by clinical research findings, and patients and prescribers must be able to trust the presented research evidence. However, this evidence can be considered valid only if the studies included in reviews and meta-analyses signify the complete publications, without any bias. (2) Recently, the reliability of much of the evidence base for several popular therapeutic and preventive interventions has been challenged due to the publication bias. (3)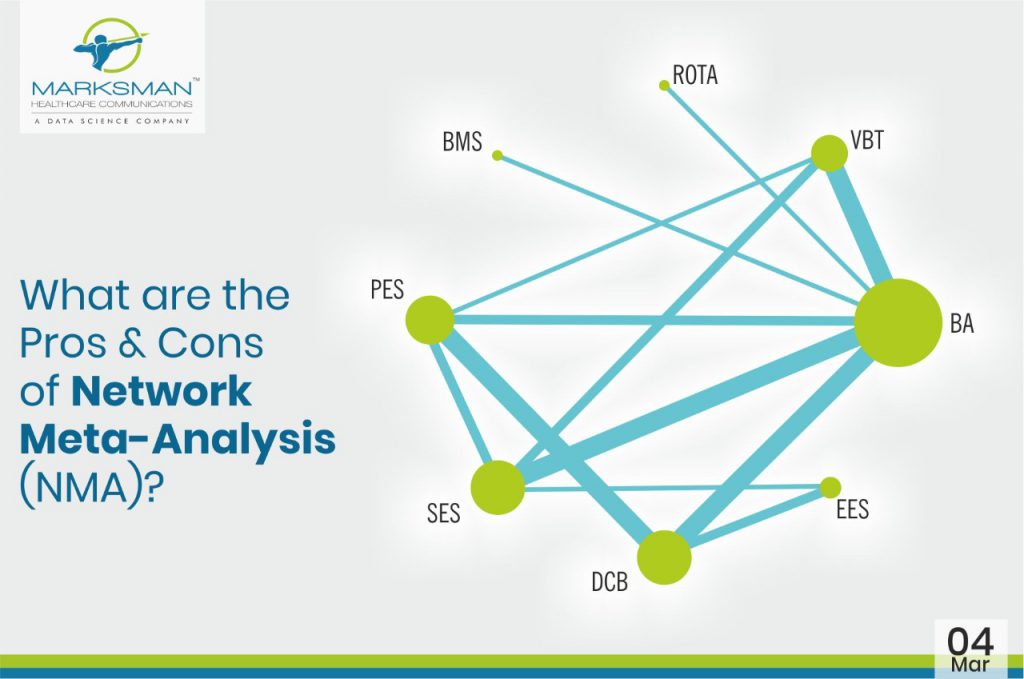
 Evidence-based medicine (EBM) is gaining wide acceptance from researchers globally as it thoroughly optimizes the latest available evidence to make informed care decisions. This involves evaluating the quality of the clinical data by critically assessing methodologies reported in publications. Moreover, EBM incorporates both clinical expertise as well as patient values. Meta-analyses of RCTs often make it among the top of the evidence hierarchy, since it’s regarded as the most valid clinical proof. Indeed, meta-analysis is a validated method to analyse and summarize knowledge by increasing the number of patients, and thus also the effective statistical power. However, there are several limitations associated with meta-analysis, which considers only pairwise comparisons. Unfortunately, head-to-head comparisons are not always available in the literature or they fail to answer a specific clinical question. This can be overcome with the help of network meta-analysis (NMA), which helps providing a global estimate of efficacy or safety of numerous experimental treatments that have not before been directly compared with adequate precision, or at all. Network meta-analysis integrates both direct and indirect effects from the entire set of evidence. Additionally, it ranks the treatments as the best or worst on the basis of valid statistical inference methods. (1)
Evidence-based medicine (EBM) is gaining wide acceptance from researchers globally as it thoroughly optimizes the latest available evidence to make informed care decisions. This involves evaluating the quality of the clinical data by critically assessing methodologies reported in publications. Moreover, EBM incorporates both clinical expertise as well as patient values. Meta-analyses of RCTs often make it among the top of the evidence hierarchy, since it’s regarded as the most valid clinical proof. Indeed, meta-analysis is a validated method to analyse and summarize knowledge by increasing the number of patients, and thus also the effective statistical power. However, there are several limitations associated with meta-analysis, which considers only pairwise comparisons. Unfortunately, head-to-head comparisons are not always available in the literature or they fail to answer a specific clinical question. This can be overcome with the help of network meta-analysis (NMA), which helps providing a global estimate of efficacy or safety of numerous experimental treatments that have not before been directly compared with adequate precision, or at all. Network meta-analysis integrates both direct and indirect effects from the entire set of evidence. Additionally, it ranks the treatments as the best or worst on the basis of valid statistical inference methods. (1)
 Today’s era of risk based, precision and personalized medicine demands clinical prediction models. Prediction modelling studies focus on two kinds of outcomes, viz. diagnosis (probability of a condition that is undetected) and prognosis (probability of developing a certain outcome in the future). (1,2) These studies develop, validate, or update a multivariable prediction model, wherein multiple predictors are used in combination to estimate probabilities to inform and often guide individual care. Moreover, evidence from literature shows both prognostic as well as diagnostic models being widely used in various medical domains and settings, (3) such as cancer, (4) neurology, (5) and cardiovascular disease. (6) Increasingly common competing prediction models can exist for the same outcome or target population, which necessitate the systematic reviews of these prediction model studies; since their coexistence may facilitate misperceptions amongst health care providers, guideline developers, and policymakers about which model to use or recommend, and in which persons or settings. (1,7)
Today’s era of risk based, precision and personalized medicine demands clinical prediction models. Prediction modelling studies focus on two kinds of outcomes, viz. diagnosis (probability of a condition that is undetected) and prognosis (probability of developing a certain outcome in the future). (1,2) These studies develop, validate, or update a multivariable prediction model, wherein multiple predictors are used in combination to estimate probabilities to inform and often guide individual care. Moreover, evidence from literature shows both prognostic as well as diagnostic models being widely used in various medical domains and settings, (3) such as cancer, (4) neurology, (5) and cardiovascular disease. (6) Increasingly common competing prediction models can exist for the same outcome or target population, which necessitate the systematic reviews of these prediction model studies; since their coexistence may facilitate misperceptions amongst health care providers, guideline developers, and policymakers about which model to use or recommend, and in which persons or settings. (1,7)
 Network meta-analysis (NMA) is a type of meta-analysis that adds an additional variable to a meta-analysis, and instead of a simple summation of trials that have evaluated the same treatment, several different treatments are compared by statistical inference.1 NMA is also referred to as mixed treatments comparison or multiple treatments comparison meta-analysis.2,3,4
Network meta-analysis (NMA) is a type of meta-analysis that adds an additional variable to a meta-analysis, and instead of a simple summation of trials that have evaluated the same treatment, several different treatments are compared by statistical inference.1 NMA is also referred to as mixed treatments comparison or multiple treatments comparison meta-analysis.2,3,4
 Every country exercises strict control on medicines’ market access. Typically, this requires successful completion and adequate presentation of results from phase I through phase III clinical trials, bringing forward the findings of medicine’s safety and efficacy. The USFDA approves approximately 40 new medicines for the US market each year through this process. (1) In India, this number is more than 100 new medicines annually; however, there is not enough published evidence on submitted applications or summaries of approved medicines. Therefore, concerns are being raised about the safety and efficacy around medicine approvals in India in the absence of appropriate clinical trials. (2,3)
Every country exercises strict control on medicines’ market access. Typically, this requires successful completion and adequate presentation of results from phase I through phase III clinical trials, bringing forward the findings of medicine’s safety and efficacy. The USFDA approves approximately 40 new medicines for the US market each year through this process. (1) In India, this number is more than 100 new medicines annually; however, there is not enough published evidence on submitted applications or summaries of approved medicines. Therefore, concerns are being raised about the safety and efficacy around medicine approvals in India in the absence of appropriate clinical trials. (2,3)
 Scoping reviews are exploratory projects that systematically map the literature on a topic, identifying key concepts, theories and sources of evidence. Scoping reviews are often conducted before full syntheses, and undertaken when feasibility of the research is considered to be a challenge, either because the relevant literature is thought to be vast and diverse (varying by methods, theoretical orientations and disciplines) and/or it is thought that little literature exists. In the scoping review, the same systematic, rigorous methodologies used by the systematic review are used to find studies and extract data. Analyses and syntheses are part of every scoping review but the depth and type of analysis are different.
Scoping reviews are exploratory projects that systematically map the literature on a topic, identifying key concepts, theories and sources of evidence. Scoping reviews are often conducted before full syntheses, and undertaken when feasibility of the research is considered to be a challenge, either because the relevant literature is thought to be vast and diverse (varying by methods, theoretical orientations and disciplines) and/or it is thought that little literature exists. In the scoping review, the same systematic, rigorous methodologies used by the systematic review are used to find studies and extract data. Analyses and syntheses are part of every scoping review but the depth and type of analysis are different.
 Health systems have developed at different speeds, and with differing degrees of complexity throughout the twentieth century, reflecting the diverse political and social conditions in each country. Notwithstanding their diversity, all systems, however, share a common reason for their existence, namely the improvement of health for their entire populations. To attain this goal a health system undertakes a series of functions, most notably, the financing and delivering of health services.
Health systems have developed at different speeds, and with differing degrees of complexity throughout the twentieth century, reflecting the diverse political and social conditions in each country. Notwithstanding their diversity, all systems, however, share a common reason for their existence, namely the improvement of health for their entire populations. To attain this goal a health system undertakes a series of functions, most notably, the financing and delivering of health services.