

Meta-analysis is a cornerstone of evidence-based research, offering a systematic approach to combine and synthesize data from multiple studies. However, as research questions become more nuanced and datasets more diverse, the complexity of meta-analyses increases significantly. This is where the Data Extraction for Complex Meta-Analysis (DECiMAL) guide comes into play, providing a structured framework to navigate these complexities.[1]
Extracting data for meta-analysis can be a complex task, especially when dealing with diverse study designs, outcomes, and data formats. Traditional data extraction methods may not be sufficient to handle the complexities of modern research, leading to potential biases and inconsistencies in the analysis. The DECiMAL guide addresses these challenges by offering a detailed methodology for data extraction, ensuring all relevant information is captured and analyzed consistently. This promotes standardization, reduces bias, and enhances transparency in the meta-analysis process, ultimately leading to more reliable and informative results. DECiMAL covers a wide range of data types, including continuous, binary, and time-to-event outcomes, as well as more complex data structures, such as multiple treatment arms and correlated outcomes. By addressing these complexities, DECiMAL helps researchers conduct rigorous and reproducible meta-analyses.[1-3]
The DECiMAL guide comprises several core components designed to tackle the complexities of meta-analyses. First, it stresses the importance of a clearly defined research question, utilizing the Population, Intervention, Comparison, and Outcome (PICO) criteria to guide the data extraction process. A comprehensive literature search is essential, and DECiMAL advocates for a systematic approach across various databases to capture all relevant studies while minimizing publication bias, with meticulous documentation of the search strategy. The guide’s detailed data extraction template captures a broad range of data points, ensuring consistency and completeness. Addressing heterogeneity is another key aspect, with DECiMAL offering guidance on statistical methods like subgroup analyses and meta-regression to understand variability between studies. For data synthesis and analysis, DECiMAL provides best practices, including the use of fixed-effect and random-effects models and a multivariate approach for diagnostic accuracy studies. It also emphasizes the assessment of bias using standardized tools and advocates for transparent reporting according to guidelines, such as PRISMA, which supports replication and enhances research credibility.[4]
The DECiMAL guide provides a detailed methodology for extracting various types of data for meta-analysis. For time-to-event data, such as cancer recurrence, hazard ratios and their uncertainties should be collected, and it should be noted if Kaplan-Meier plots or life tables are reported. For rate data, like migraine episode frequency, the total number of person-years at risk should be collected. If this information is not available, the average length of follow-up and the total number of patients at study end can be used to approximate person-years. Binary and categorical variables should use numerical coding for responses and additional coding for other responses, while both numbers of patients randomized and those completing the trial should be extracted. Continuous and ordinal variables should be consistently reported in chosen units, with both final values and changes from the baseline being combined if baselines are equal. The guide ensures comprehensive data collection and helps identify and address potential issues early on, enhancing the consistency and accuracy of complex meta-analyses.[4]
While DECiMAL provides a comprehensive framework for data extraction, it has certain limitations. For instance, it does not delve into specific statistical techniques for handling missing data or converting summary statistics. Additionally, while DECiMAL is primarily designed for aggregate data meta-analyses, it may not be directly applicable to individual patient data meta-analyses. The guide primarily addresses considerations related to data extraction for subsequent meta-analyses but provides limited information on the practical and technical aspects of data extraction itself. Furthermore, DECiMAL is designed specifically for data extraction in aggregate data meta-analyses, and its methods do not apply to individual patient data meta-analyses.[4]
The DECiMAL guide marks significant progress in meta-analysis, especially for handling complex datasets. By standardizing data extraction, addressing heterogeneity, and enhancing transparency, DECiMAL ensures that meta-analytical results are robust and reliable. With the increasing volume and complexity of research data, adopting comprehensive tools like DECiMAL will be essential for preserving the integrity and effectiveness of meta-analyses. For researchers undertaking complex meta-analyses, DECiMAL provides a structured approach to navigating the challenges of data extraction and analysis. Following its guidelines can improve the quality and impact of research findings, offering valuable contributions to the scientific community.
Become A Certified HEOR Professional – Enrol yourself here!
References:
- Brown SA, Upchurch SL, Acton GJ. A framework for developing a coding scheme for meta-analysis. West J of Nurs Res. 2003;25:205–22.
- Centre for Evidence-Based Medicine. Data Extraction Tips: Meta-Analysis [Internet]. Oxford: University of Oxford. 2023; Available from: https://www.cebm.ox.ac.uk/resources/data-extraction-tips-meta-analysis.
- Effective Practice and Organisation of Care (EPOC). Data collection form. EPOC Resources for review authors. Norwegian Knowledge Centre for the Health Services. 2013;Available from: http://epoc.cochrane.org/epoc-specific-resources-review-authors.
- Pedder H, Sarri G, Keeney E, Nunes V, Dias S. Data extraction for complex meta-analysis (DECiMAL) guide. Syst Rev. 2016 Dec 13;5(1):212. 5. Afifi M, Stryhn H, Sanchez J. Data extraction and comparison for complex systematic reviews: a step-by-step guideline and an implementation example using open-source software. Syst Rev. 2023 Dec 1;12(1):226.



 Systematic reviews (SRs) are the embodiment of the evidence-based approaches, and they have reformed clinical decision-making in almost all therapy areas. The approach of SRs was essentially developed to fulfil the need of the medical practitioners to obtain precise and consistent information about the efficacy and safety of a clinical intervention, diagnostic procedure, or a prognostic marker from a pool of evidence, which is apparently full of contradiction, heterogeneity and bias.(1) Although SRs and meta-analyses are robust and detail-oriented, they’re both resource intense, with a limited scope of outcomes.(2) In order to cater to a range of needs from the stakeholders, the SR approach has branched within the realm of evidence synthesis. For instance, rapid reviews provide for more urgent deadlines but may not follow all the methods of an SR,(3) scoping reviews include larger bodies of evidence, not requiring a detailed synthesis,(4) and realist reviews focus on the assessment of the functions of complex interventions, often comprising of evidence excluded from classic SRs.(5, 6)
Systematic reviews (SRs) are the embodiment of the evidence-based approaches, and they have reformed clinical decision-making in almost all therapy areas. The approach of SRs was essentially developed to fulfil the need of the medical practitioners to obtain precise and consistent information about the efficacy and safety of a clinical intervention, diagnostic procedure, or a prognostic marker from a pool of evidence, which is apparently full of contradiction, heterogeneity and bias.(1) Although SRs and meta-analyses are robust and detail-oriented, they’re both resource intense, with a limited scope of outcomes.(2) In order to cater to a range of needs from the stakeholders, the SR approach has branched within the realm of evidence synthesis. For instance, rapid reviews provide for more urgent deadlines but may not follow all the methods of an SR,(3) scoping reviews include larger bodies of evidence, not requiring a detailed synthesis,(4) and realist reviews focus on the assessment of the functions of complex interventions, often comprising of evidence excluded from classic SRs.(5, 6)
 During the course of any research, most of the relevant literature pertaining to a research question is retrieved though searching of recognised databases. However, in addition to this, searching of grey literature can add value to the depth of the research by providing information from varied sources. Grey literature search is an important, but often ignored, part of systematic literature review and data synthesis, especially in the medical research.
During the course of any research, most of the relevant literature pertaining to a research question is retrieved though searching of recognised databases. However, in addition to this, searching of grey literature can add value to the depth of the research by providing information from varied sources. Grey literature search is an important, but often ignored, part of systematic literature review and data synthesis, especially in the medical research.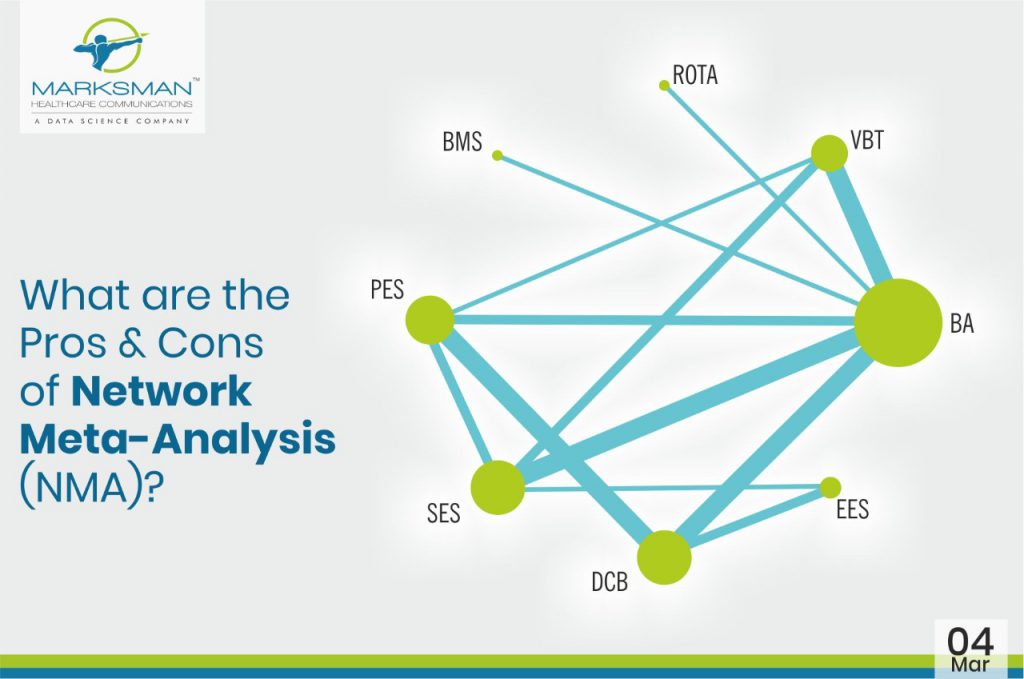
 Evidence-based medicine (EBM) is gaining wide acceptance from researchers globally as it thoroughly optimizes the latest available evidence to make informed care decisions. This involves evaluating the quality of the clinical data by critically assessing methodologies reported in publications. Moreover, EBM incorporates both clinical expertise as well as patient values. Meta-analyses of RCTs often make it among the top of the evidence hierarchy, since it’s regarded as the most valid clinical proof. Indeed, meta-analysis is a validated method to analyse and summarize knowledge by increasing the number of patients, and thus also the effective statistical power. However, there are several limitations associated with meta-analysis, which considers only pairwise comparisons. Unfortunately, head-to-head comparisons are not always available in the literature or they fail to answer a specific clinical question. This can be overcome with the help of network meta-analysis (NMA), which helps providing a global estimate of efficacy or safety of numerous experimental treatments that have not before been directly compared with adequate precision, or at all. Network meta-analysis integrates both direct and indirect effects from the entire set of evidence. Additionally, it ranks the treatments as the best or worst on the basis of valid statistical inference methods. (1)
Evidence-based medicine (EBM) is gaining wide acceptance from researchers globally as it thoroughly optimizes the latest available evidence to make informed care decisions. This involves evaluating the quality of the clinical data by critically assessing methodologies reported in publications. Moreover, EBM incorporates both clinical expertise as well as patient values. Meta-analyses of RCTs often make it among the top of the evidence hierarchy, since it’s regarded as the most valid clinical proof. Indeed, meta-analysis is a validated method to analyse and summarize knowledge by increasing the number of patients, and thus also the effective statistical power. However, there are several limitations associated with meta-analysis, which considers only pairwise comparisons. Unfortunately, head-to-head comparisons are not always available in the literature or they fail to answer a specific clinical question. This can be overcome with the help of network meta-analysis (NMA), which helps providing a global estimate of efficacy or safety of numerous experimental treatments that have not before been directly compared with adequate precision, or at all. Network meta-analysis integrates both direct and indirect effects from the entire set of evidence. Additionally, it ranks the treatments as the best or worst on the basis of valid statistical inference methods. (1)
 Network meta-analysis (NMA) is a type of meta-analysis that adds an additional variable to a meta-analysis, and instead of a simple summation of trials that have evaluated the same treatment, several different treatments are compared by statistical inference.1 NMA is also referred to as mixed treatments comparison or multiple treatments comparison meta-analysis.2,3,4
Network meta-analysis (NMA) is a type of meta-analysis that adds an additional variable to a meta-analysis, and instead of a simple summation of trials that have evaluated the same treatment, several different treatments are compared by statistical inference.1 NMA is also referred to as mixed treatments comparison or multiple treatments comparison meta-analysis.2,3,4