

Patient Preference Information (PPI) has emerged as a powerful tool, gaining recognition in the healthcare industry for its multifaceted ability to enhance patient-centered care, refine clinical trial design, and inform crucial treatment decisions. The drive towards patient-centered care has become a hallmark of modern healthcare, emphasizing the need to tailor healthcare decisions and practices according to patients’ values and preferences. In this context, PPI assumes a pivotal role by providing invaluable insights into patients’ authentic desires and requirements. Furthermore, PPI has the potential to revolutionize clinical research and treatment strategies by actively incorporating the patient’s perspective into the decision-making process.[1]
The advantages of incorporating PPI into clinical research are manifold, including enhanced patient recruitment and retention, refined trial design, and elevated patient satisfaction. Clinical trials stand as the bedrock of advancing medical knowledge and ushering in new treatments. However, traditional RCTs are often criticized as being physician-centric, research-oriented, and being executed in a ‘controlled setting’ without much importance to patient preferences.[2] The integration of PPI into clinical trial design can potentially improve the patient-centricity of the research [3]. For example, in a clinical trial, patients may be given the choice between two treatment regimens with differing efficacy and side effect profiles: hypothetically, patients can be asked to select either an option with a lower efficacy but better safety, or an alternative with a higher efficacy but not-yet-completely-known safety profile. Based on these preferences, randomization can be carried out: a design sometimes referred to as ‘preference-based randomization’. This ensures that the selected treatment aligns closely with the patient’s preferences and lifestyle.[4] Such preference-based randomization allows patients to articulate their treatment preferences, enabling researchers to allocate treatments accordingly. This approach not only enhances patient engagement but also holds the potential to improve treatment adherence, thereby yielding more accurate outcomes.[1-3]
PPI extends its influence beyond the confines of clinical trials, exerting a substantial impact on the daily landscape of patient care. Central to the concept of patient-centered care is the notion of treating the patient as an active and engaged participant in their healthcare journey. In this context, PPI serves as a vital connective bridge that facilitates seamless communication and collaboration between healthcare providers and patients, bridging the gap between medical expertise and individual values and choices.[1] PPI equips healthcare providers with profound insights into patients’ values, preferences, and goals, facilitating the creation of personalized care plans that harmonize with the patient’s desires. For instance, an older patient facing a terminal illness may prioritize the quality of life over aggressive treatments: accordingly, PPI can steer the development of a care plan that honors this preference.[1,2]
On the other end of the table, PPIs can also empower patients. The PPI gathering process can make acquaint the patient with comprehensive information regarding their treatment options and possible outcomes, making them more inclined to actively partake in decisions regarding their care, thus championing shared decision-making and fostering enhanced collaboration between patients and healthcare providers to make well-informed choices. For instance, a patient diagnosed with breast cancer may harbor strong preferences concerning the timing of surgery. Here, PPI can guide discussions regarding the appropriate treatment timeline. This collaborative approach often translates into enhanced treatment adherence and heightened patient satisfaction.[1,2]
Regulatory agencies have come to recognize the pivotal role of PPI in healthcare decision-making. These agencies are increasingly incorporating PPI into their evaluations of novel drugs and medical devices. For instance, the USFDA developed a set of guidance in 2020 regarding the collection and use of PPI in regulatory decision-making, underscoring its significance in benefit-risk assessments. Similarly, the European Medicines Agency (EMA) is actively exploring the incorporation of patient preferences in benefit-risk assessments. Additionally, Health Canada has initiated the Patient and Public Engagement Initiative, involving patients in drug approval processes. The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK values patient input and engagement in its regulatory activities, while the Therapeutic Goods Administration (TGA) in Australia is incorporating patients’ perspectives, particularly in medical device approvals. This information informs regulatory decisions and ensures that healthcare interventions align with patient preferences and expectations.[5-11]
All said, incorporating PPI into clinical research presents several significant challenges. First and foremost is the need for standardization in the collection and analysis of PPI, as patient preferences can vary widely across different contexts. Ensuring that the preferences of trial participants accurately represent the broader patient population is another challenge, as volunteer biases can skew data. Moreover, using PPI for randomization in RCTs may introduce bias, as it could lead to a non-representative sample if patients with strong preferences self-select into certain treatment arms. Ethical considerations, resource intensiveness, integration with regulatory requirements, interpreting and applying PPI data, patient education, and engagement are all practical challenges that must be addressed. Finally, achieving regulatory acceptance and standardization of PPI methods and findings across regions and healthcare systems remains a critical hurdle.[12]
The use of PPIs in routine clinical practice is associated with a distinct set of challenges. These include the seamless integration of PPI data into electronic health records and clinical workflows, the importance of upholding patient privacy and securing informed consent for its use. Other complexities include the need for proper interpretation and application of PPI data in individual patient care decisions and the requirement for training healthcare providers to communicate and utilize PPI effectively. Additionally, allocating adequate time and resources in busy clinical settings, fostering patient engagement in sharing their preferences, and developing standardized methods for collecting also pose complications to the use of PPIs in healthcare. Overcoming these challenges necessitates collaboration among stakeholders to harness the potential benefits of PPI in enhancing the relevance and patient-centeredness of clinical research and healthcare decision-making.[12]
In conclusion, PPI is an indispensable and versatile tool in healthcare, both in research and routine healthcare delivery, as indicated by the growing acknowledgment of PPIs by regulatory agencies. Its manifold applications encompass the enhancement of clinical trial design, the augmentation of patient-centered care, and the facilitation of treatment selection, all fostering an enhancement of patient-centered care and medical research. PPI empowers patients to occupy a central role in their healthcare decisions, ultimately culminating in improved patient outcomes and heightened patient satisfaction.
Become A Certified HEOR Professional – Enrol yourself here!
References
- McPherson K, Chalmers I. Incorporating patient preferences into clinical trials. Information about patients’ preference must be obtained first. BMJ. 1998 Jul 4;317(7150):78; author reply 78-9.
- Wasmann KA, Wijsman P, van Dieren S, Bemelman W, Buskens C. Partially randomised patient preference trials as an alternative design to randomised controlled trials: systematic review and meta-analyses. BMJ Open. 2019 Oct 16;9(10):e031151.
- Lambert MF, Wood J. Incorporating patient preferences into randomized trials. Journal of clinical epidemiology. 2000 Feb 1;53(2):163-6.
- Kowalski CJ, Mrdjenovich AJ. Patient preference clinical trials: why and when they will sometimes be preferred. Perspectives in biology and medicine. 2013;56(1):18-35.
- Sharma NS. Patient centric approach for clinical trials: Current trend and new opportunities. Perspect Clin Res. 2015 Jul-Sep;6(3):134-8.
- Marshall, Deborah A. “Brief Overview of Patient Preference Information (PPI).” FDA Committee. PowerPoint Presentation. March 2021. https://www.fda.gov/media/146925/download.
- Irony T, Ho M, Christopher S, Levitan B. Incorporating patient preferences into medical device benefit-risk assessments. Statistics in Biopharmaceutical Research. 2016 Jul 2;8(3):230-6.
- Mühlbacher AC, Juhnke C, Beyer AR, Garner S. Patient-focused benefit-risk analysis to inform regulatory decisions: the European Union perspective. Value in Health. 2016 Sep 1;19(6):734-40.
- Weeks L, Polisena J, Scott AM, Holtorf AP, Staniszewska S, Facey K. Evaluation of patient and public involvement initiatives in health technology assessment: a survey of international agencies. International journal of technology assessment in health care. 2017;33(6):715-23.
- Aiyegbusi OL, Cruz Rivera S, Oliver K, Manna E, Collis P, King-Kallimanis BL, Bhatnagar V, Herold R, Hopkins J, Campbell L, Croker A. The opportunity for greater patient and public involvement and engagement in drug development and regulation. Nature Reviews Drug Discovery. 2023 May;22(5):337-8.
- Russell TG, Jones AF. Implications of regulatory requirements for smartphones, gaming consoles and other devices. Journal of physiotherapy. 2011 Jan 1;57(1):5-7.
- Selman LE, Clement C, Douglas M, et al. Patient and public involvement in randomised clinical trials: a mixed-methods study of a clinical trials unit to identify good practice, barriers and facilitators. Trials. 2021 Dec;22:1-4.

 Health technology assessment (HTA) is a process that evaluates the safety, efficacy, and cost-effectiveness of medical technologies, such as drugs, medical devices, and diagnostic tests, in order to inform decision-making about their use in healthcare. It is a multidisciplinary approach that explores health technologies from clinical, economic, and the larger societal viewpoint. (1)
Health technology assessment (HTA) is a process that evaluates the safety, efficacy, and cost-effectiveness of medical technologies, such as drugs, medical devices, and diagnostic tests, in order to inform decision-making about their use in healthcare. It is a multidisciplinary approach that explores health technologies from clinical, economic, and the larger societal viewpoint. (1)
 Living systematic literature reviews (SLRs) are a type of SLRs that are continually updated by periodically including relevant new evidence as and when it becomes available. SLRs are often considered to occupy the top of the evidence pyramid because they synthesize evidence from different sources and present a summary of the evidence, thus enabling clinical and policy-level decision-making.
Living systematic literature reviews (SLRs) are a type of SLRs that are continually updated by periodically including relevant new evidence as and when it becomes available. SLRs are often considered to occupy the top of the evidence pyramid because they synthesize evidence from different sources and present a summary of the evidence, thus enabling clinical and policy-level decision-making.
 Improvements in healthcare digitalization and accelerated regulatory approvals of novel interventions have boosted the possibilities for gathering real-world data (RWD) and using the resultant real-world evidence (RWE) to support the generalizability, efficacy, and safety of interventions and medical devices, assisting healthcare decision-makers and policymakers.
Improvements in healthcare digitalization and accelerated regulatory approvals of novel interventions have boosted the possibilities for gathering real-world data (RWD) and using the resultant real-world evidence (RWE) to support the generalizability, efficacy, and safety of interventions and medical devices, assisting healthcare decision-makers and policymakers.
 The world today is observing an exponential growth in the volume and variety of the real-world data (RWD). Thanks to the technological advancements and the rise in the use of integrated electronic medical records (EMRs), RWD is ever more accessible and applicable in the regulatory domain as well as outcomes research. The evidence from randomized controlled trials (RCTs) is still undoubtedly the gold standard for assessing treatment efficacy; however, the interest and potential for adapting RWD into real-world evidence (RWE) is on the rise. This can prove extremely beneficial to make informed healthcare decisions. (1)
The world today is observing an exponential growth in the volume and variety of the real-world data (RWD). Thanks to the technological advancements and the rise in the use of integrated electronic medical records (EMRs), RWD is ever more accessible and applicable in the regulatory domain as well as outcomes research. The evidence from randomized controlled trials (RCTs) is still undoubtedly the gold standard for assessing treatment efficacy; however, the interest and potential for adapting RWD into real-world evidence (RWE) is on the rise. This can prove extremely beneficial to make informed healthcare decisions. (1)
 Patient Records Abstraction (PRA) is a process done manually by searching through a medical record to identify data required for a particular or secondary use. It consists of direct matching of information found in the record to the data required, but also includes operations on the data such as categorizing, coding, transforming, interpreting, summarizing, and calculating. The abstraction, in the end, summarizes information about a patient for a specific secondary data use. (1) PRA typically involves reviewing patient files and abstracting (i.e., extracting) key data, which are then entered into electronic files. (2) Depending on the measure or purpose, there can be different sources for data collection such as paper medical records, electronic medical records (EMR), patient surveys, administrative databases, etc.
Patient Records Abstraction (PRA) is a process done manually by searching through a medical record to identify data required for a particular or secondary use. It consists of direct matching of information found in the record to the data required, but also includes operations on the data such as categorizing, coding, transforming, interpreting, summarizing, and calculating. The abstraction, in the end, summarizes information about a patient for a specific secondary data use. (1) PRA typically involves reviewing patient files and abstracting (i.e., extracting) key data, which are then entered into electronic files. (2) Depending on the measure or purpose, there can be different sources for data collection such as paper medical records, electronic medical records (EMR), patient surveys, administrative databases, etc.
 Healthcare decision making is usually characterized by a low degree of transparency. The demand for transparent decision processes can be fulfilled only when assessment, appraisal and decisions about health technologies are performed under a systematic construct of benefit assessment. The benefit of an intervention is often multidimensional and, thus, must be represented by several decision criteria. Complex decision problems require an assessment and appraisal of various criteria; therefore, a decision process that systematically identifies the best available alternative and enables an optimal and transparent decision is needed. Complexity in the healthcare decisions is inevitable, whether a high-level decision, such as that made by a budget holder, allocating limited resources across treatments, or at the micro-level, such as a patient’s decision on the best treatment alternative.
Healthcare decision making is usually characterized by a low degree of transparency. The demand for transparent decision processes can be fulfilled only when assessment, appraisal and decisions about health technologies are performed under a systematic construct of benefit assessment. The benefit of an intervention is often multidimensional and, thus, must be represented by several decision criteria. Complex decision problems require an assessment and appraisal of various criteria; therefore, a decision process that systematically identifies the best available alternative and enables an optimal and transparent decision is needed. Complexity in the healthcare decisions is inevitable, whether a high-level decision, such as that made by a budget holder, allocating limited resources across treatments, or at the micro-level, such as a patient’s decision on the best treatment alternative.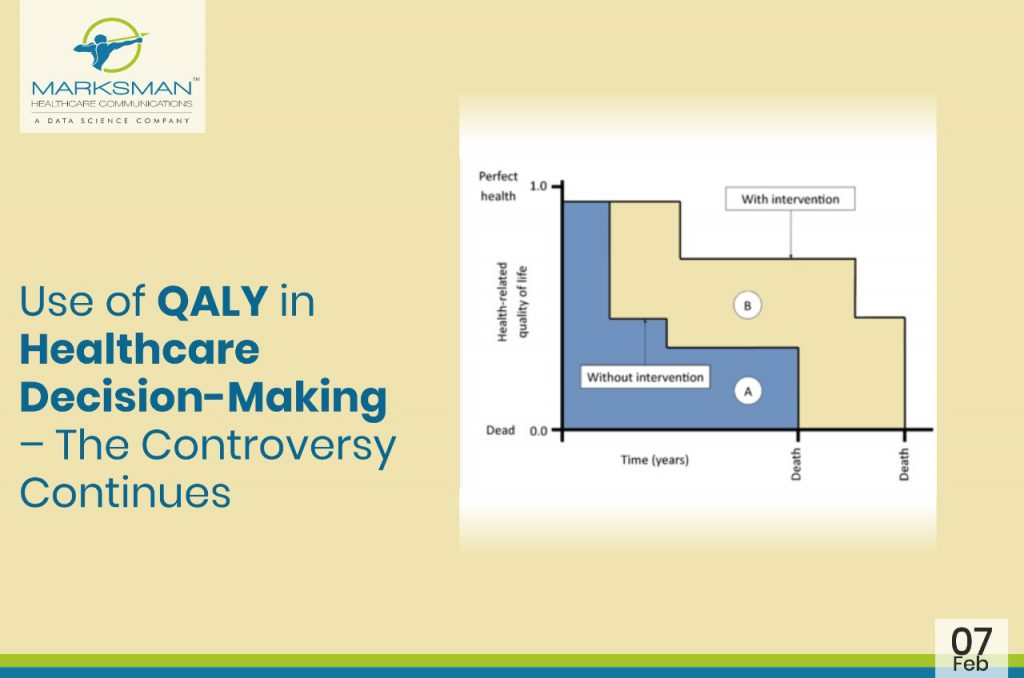
 In many parts of the world, the value of medicines is measured by a unit called ‘Quality-Adjusted Life Year’ (QALY), a metric that health economists and others use to quantify the health benefits generated by a particular treatment. QALYs are often used by state-run health systems in many countries to help decide which drugs to cover.
In many parts of the world, the value of medicines is measured by a unit called ‘Quality-Adjusted Life Year’ (QALY), a metric that health economists and others use to quantify the health benefits generated by a particular treatment. QALYs are often used by state-run health systems in many countries to help decide which drugs to cover.