

Quality-Adjusted Life Years (QALY) is an important concept in health technology assessment since it provides a comprehensive assessment of the impact of diverse healthcare interventions by combining the length and quality of life into a single measure. QALY is measured by integrating life expectancy and quality of life (QoL). Various methods are employed to assess QoL, including structured questionnaires (such as generic questionnaires like EQ-5D, or disease-specific questionnaires), and preference-based interviews like time trade-off (TTO), standard gamble (SG), or visual analog scale (VAS).[1]
The extensive use of QALYs is a result of several advantages. QALYs offer a standardized metric for comparing the effectiveness of various health interventions used in the management of diverse health conditions. This common scale helps policymakers and healthcare professionals prioritize interventions within a shared framework. The use of QALY can also promote objectivity in decision-making by treating individuals equally and avoiding biases related to age or health status. Additionally, it is possible to evaluate changes in health status over time by using QALYs, acknowledging the dynamic nature of health conditions.[1,2]
QALY essentially involves evaluation and quantification of QoL through various means: since this results exclusively from a patient’s subjective assessment of the outcome of an intervention, QALYs also represent a patient-centric view of treatment outcomes, contrasting to the physician-centered efficacy and safety measures. This inclusion ensures a broader and more comprehensive perspective, aligning with the principle that public funding drives new treatments. QALY also contributes immensely to cost-utility analysis by allowing the calculation of cost-per-QALY, thereby helping policymakers navigate the complex landscape of resource allocation; this enables the maximization of health outcomes within budget constraints.[1,2]
Despite these advantages, the QALY approach is not without its criticisms. The value dependency of QALY introduces subjectivity, with the choice of perspective (patient, service provider, or general public) impacting the analysis. Critics argue that disease-non-specific (generic) QoL tools like EQ-5D, while having the advantage of enabling comparison between diverse conditions, may oversimplify health states, especially in mental health cases, potentially neglecting important aspects valued by patients. Additionally, concerns about equity arise as QALY assumes equal social value for all, potentially leading to inequitable weighting based on characteristics such as sex and socioeconomic standing.[3,4]
The age neutrality of QALY and its focus primarily on health service costs are additional drawbacks. These limitations raise questions about their universality and applicability across diverse healthcare scenarios. The discounting of future benefits also sparks ethical concerns regarding the fair distribution of healthcare resources over time. Decision-makers must grapple with these challenges, balancing the advantages and disadvantages of the QALY approach when employing it as a metric for healthcare decision-making.[3,4]
In response to the acknowledged limitations of the QALY approach, several alternative metrics have been proposed, each presenting a distinct set of advantages and limitations. These alternatives aim to offer more comprehensive and nuanced evaluations of healthcare interventions, recognizing the diverse aspects of health outcomes. The willingness to Pay (WTP) approach serves as an alternative by incorporating individual preferences, and addresses a criticism of QALY for overlooking individual values. However, the WTP exercise is better suited for economic evaluations than for pure QoL analyses. Conducting a comprehensive WTP interview demands additional expertise in economic modeling, surveys, and analysis. WTP questionnaires also often involve more items and scale points, contributing to implementation complexities. These factors collectively make WTP a time and resource-intensive method.[5,6]
Another metric seeking to address QALY’s limitations by focusing on a different aspect of well-being is Quality-Adjusted Time Without Symptoms or Toxicity (Q-TWIST); however, this approach has challenges related to complexity and applicability, potentially restricting its application to a narrower range of healthcare interventions. Wellbeing-Adjusted Life Year (WELLBY) takes a broader approach by encompassing happiness and life satisfaction alongside health considerations, thereby addressing the limitation of QALY’s narrow focus on health outcomes; on the flip side, WELLBY faces challenges related to subjectivity and standardization, which could impact its reliability and consistency across evaluations.[5,6]
Disability-Adjusted Life Year (DALY) offers a comprehensive evaluation by considering both premature mortality and years lived with disability, presenting a holistic perspective on disease burden. However, DALY’s criticisms include complexities in measuring disability, thereby potentially not capturing overall well-being satisfactorily, akin to looking at a ‘negative’ aspect to capture a ‘positive’ measure. Next, the Multi-Criteria Decision Analysis (MCDA) is a measure that evaluates options with conflicting criteria and selects the best solution accommodating complexity and stakeholder involvement. However, MCDA is often considered subjective and inconsistent and is also quite resource-intensive. Finally, the equal value of Life Years Gained (evLYG) strives for equitable assessments by considering age and baseline health, addressing QALY’s potential age bias; however, there are challenges in determining equal value across diverse health conditions.[5,6]
The choice of a specific metric to measure QoL and QALY hinges on evaluation goals, contextual nuances, and stakeholder values. The ongoing evolution of healthcare value assessment methodologies reflects the dynamic nature of the field, with researchers and policymakers continually exploring and refining approaches to better capture the complexity of healthcare outcomes and their societal implications.[5,6]
While numerous alternatives are available, QALY is undoubtedly the most frequently used metric despite its drawbacks and criticisms. The advantages of QALY, such as its comprehensive measurement, comparative analysis capabilities, and standardized metric, make it a practical tool for assessing the value of healthcare interventions. However, the subjectivity in quality assessment and limited applicability in certain scenarios might prompt consideration of alternative metrics discussed above. Ultimately, the quest for a complete tool for value assessment requires ongoing research, collaboration, and a commitment to refining existing methodologies to better align with the diverse and complex nature of healthcare interventions and outcomes.
Become A Certified HEOR Professional – Enrol yourself here!
References
- Whitehead SJ, Ali S. Health outcomes in economic evaluation: the QALY and utilities. British medical bulletin. 2010 Dec 1;96(1):5-21.
- Prieto L, Sacristán JA. Problems and solutions in calculating quality-adjusted life years (QALYs). Health Qual Life Outcomes. 2003 Dec 19;1:80.
- Brazier J, Tsuchiya A. Improving cross-sector comparisons: going beyond the health-related QALY. Applied health economics and health policy. 2015 Dec;13:557-65.
- Pettitt DA, Raza S, Naughton B, Roscoe A, Ramakrishnan A, Ali A, Davies B, Dopson S, Hollander G, Smith J, Brindley D. The limitations of QALY: a literature review. Journal of Stem Cell Research and Therapy. 2016;6(4).
- Carlson JJ, Brouwer ED, Kim E, Wright P, McQueen RB. Alternative Approaches to Quality-Adjusted Life-Year Estimation Within Standard Cost-Effectiveness Models: Literature Review, Feasibility Assessment, and Impact Evaluation. Value Health. 2020 Dec;23(12):1523-1533.
- Gafni A. Alternatives to the QALY measure for economic evaluations. Supportive care in cancer. 1997 Mar;5:105-11.

 Health utilities are cardinal values in identifying an individual’s preference for different health outcomes. Health utilities are transformed to Quality Adjusted Life Years (QALYs) to enable comparisons between health interventions in cost-utility analysis in Pharmacoeconomics. Health utilities are measured using various utility ‘instruments’, which can be either generic (that is, can be applied to all diseases) or disease-specific.[1] Utility instruments are most of the times well-crafted questionnaires designed to capture and score the utility and thereby calculate the overall quality of life. Since the comparison of utility gains are often used in healthcare policy setting, it is essential that the instruments used to measure the utilities are rigorously validated.
Health utilities are cardinal values in identifying an individual’s preference for different health outcomes. Health utilities are transformed to Quality Adjusted Life Years (QALYs) to enable comparisons between health interventions in cost-utility analysis in Pharmacoeconomics. Health utilities are measured using various utility ‘instruments’, which can be either generic (that is, can be applied to all diseases) or disease-specific.[1] Utility instruments are most of the times well-crafted questionnaires designed to capture and score the utility and thereby calculate the overall quality of life. Since the comparison of utility gains are often used in healthcare policy setting, it is essential that the instruments used to measure the utilities are rigorously validated.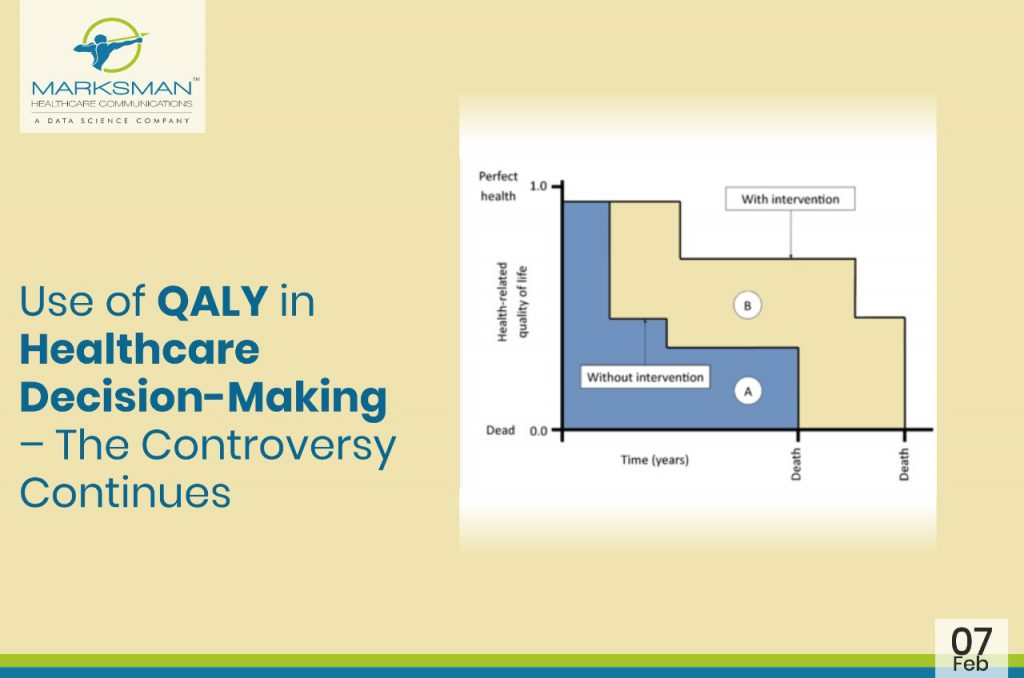
 In many parts of the world, the value of medicines is measured by a unit called ‘Quality-Adjusted Life Year’ (QALY), a metric that health economists and others use to quantify the health benefits generated by a particular treatment. QALYs are often used by state-run health systems in many countries to help decide which drugs to cover.
In many parts of the world, the value of medicines is measured by a unit called ‘Quality-Adjusted Life Year’ (QALY), a metric that health economists and others use to quantify the health benefits generated by a particular treatment. QALYs are often used by state-run health systems in many countries to help decide which drugs to cover.